There is an op-ed in today’s daily rag slamming Kamala
Harris’ talking points on health care, principally by using the same blatant
untruth most anti-single payer talking heads use. It was written by the former
Lt Governor of NY, who now lobbies for conservative issues, and one supposes, for
the Health Care and Pharma providers. The argument and the falsehood, is
generally (and this was) a variation on this theme:
“Medicare for all (or some relatively equivalent single
payer plan) would never work because Medicare only pays about 90% of the
charged amount for most procedures, and many hospitals couldn’t afford to
operate on that income.” Sounds realistic, right? We all see our bills (if we
have insurance) and we all see “amount billed,” “amount allowed” and “amount
payed.”
The big lie
here, and it’s a lie by implication, revolves not around what is said, but by
what isn’t. It’s true that Medicare
never pays the “list” price (call it retail, if it sounds easier to understand)
for essentially every billed medical procedure. What the writer omits is that the
exact same thing is true for private insurers as well. Understand what I’m
saying: While Medicare pays less than the retail amount, so do private insurers.
The crucial difference is that Medicare is consistent, while insurance
companies jealously regard as confidential the sweetheart deals negotiated with
providers which are, in some cases, actually better (less) than Medicare. These
lower negotiated rates also vary from insurer to insurer. Added to that is the
other dirty little secret, of which I have written exhaustively elsewhere,
which is that drug prices are not, by law, negotiated by Medicare. Someone -
Medicare, or patient co-pay, pays full price for meds.
Hospitals “pad”
bills with outrageously inflated drug, procedural, and room charges which they
never really expect to collect.
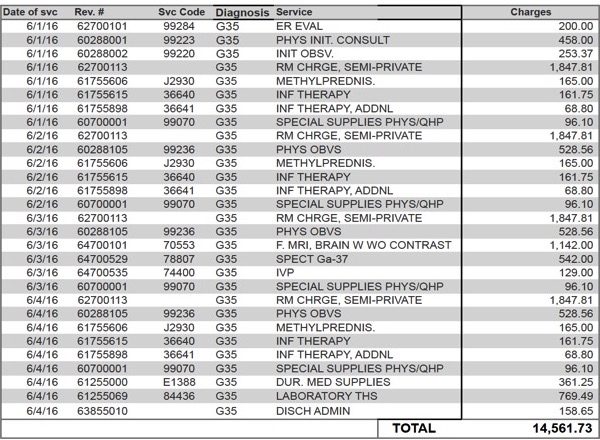
Note the entries on the above discharge bill for:
service
code J2930 - Methylprednisolone – this is about $5 dollars’ worth of meds
billed at $165 every time administered.
Phys OBVS – every time the doctor looked in (“observed”,
this isn’t procedures) the bill was $528!
The room is billed at $1847 daily. I find it amazing that
the room “charge” is $700 more each day than the billed cost of the MRI!
And finally, the last entry: “discharge admin $158.65”. Wow,
that must be some clerk!
These and all costs like these are billed as an exercise in,
hopefully, actually having a patient with no insurance and lots of money, since
that’s the only way that amount will actually be paid. The big lie in the op-ed
is that single payer is more expensive. It could be if private insurance actually
paid “list price” but they simply don’t. Never have. Add to this the great
reduction in real admin costs of billing only one entity with one universal fee
schedule, and finally, repeal, or amend, Medicare, part D to allow Medicare to
negotiate drug prices - you know, like every other insurer in America does? I
did the math in another essay some time
ago and conclude that (admittedly a rough, but realistic, estimate, since
actual data would require a Cray computer to analyze) that simply giving
Medicare/Medicaid the same leverage with Big Pharma that all private insurers and
hospitals already have would result in about a $5 billion annual reduction in
Medicare /Medicaid spending on drugs alone!
Administrative
costs, meanwhile, account for 8 percent of total national health expenditures
in the U.S. For the other countries, they ranged from 1 percent to 3 percent.
Health care professionals in America also reported a higher level of
“administrative burden.” A survey showed that a significant portion of doctors
call the time they lose to issues surrounding insurance claims and reporting
clinical data a major problem.
As for the drug market, the U.S. spent $1,443 per capita on
pharmaceuticals. The average pharmaceutical spending of 11 European OECD countries came
to $749 per capita. One myth, popular now, is that drugs are “better” from US
manufacturers, which ignores the fact than several US manufacturers make their
product by contract overseas anyway.
We all, or at
least many, if not most, of us pay for health care in various ways. So do most
employers. We, as consumers, pay some of that cost in every product we buy. We
also, while working, receive less in a pay envelope because of heath care
insurance costs paid by us as employees. We are constantly abused by drug
companies which Congress has the ability, but not the balls to rein in.
Want a good
start? Enact legislation that stipulates that in the process of getting FDA
approval, the manufacturer of a new drug must show total cost of development
and manufacturing, offset by NIH grants, if any. This, because about 40% of
newly approved drugs in the US have been developed with some degree of, or even
total, Federal funding. Allow a
reasonable, but fixed profit margin and mandate that, for the life of the
patent, the price cannot be increased more than the CPI increase.
Pharma is industry
which has net profits annually which run consistently as much as five to six
times the average for US corporations. So, what do these net profits do, beside
pay dividends (some, like Merck, as high as 7.5% + annually)? Well, in days
gone by, we simply accepted that these profits fueled research and development,
which may have been true. Not so today, however since, currently and for the
past decade or more, the largest expenditure of all major Big Pharma corporations
is Advertising. In 2016, Pharma spent
just under $10 billion on DTC (direct to consumer advertising) and another $20
billion in marketing to healthcare professionals. Only the US and New Zealand
allow DTC advertising. Now, do we see
why your physician may change your prescription, citing vague generalities? R& D, and shareholder profits share the
rest, with Lobbying around $25 million or more annually. If you care to do the
math, that’s just over $46,000 for every single member of Congress!
A change to
single payer system would be difficult, not because of the logistics, since Medicare
is already a single payer system, but because of entrenched interests. Essentially
all “Medicare isn’t cheaper” studies are funded by conservative, and/or status
quo vested interests and use current Medicare cost per patient estimates, which
due to the age of the patients involved are significantly higher than the
population as a whole. Even so, these folks do such shenanigans as adding the
cost of the IRS collecting Medicare payments for all payees and counting them,
as admin costs, while employers’ admin costs are ignored for private plans,
This also ignores the fact that private plans still can, to an extent, “cherry-pick”
clients.
Assuming a level playing field, using a spectrum of ages representative
of the entire population, Medicare’s admin costs would be (are) significantly
less than Private plans, who are able to “dump” seniors onto Medicare. Ask
yourself one final question. If Medicare is more expensive, why are so many
Health Insurers making money, even with higher admin costs, with “Medicare Advantage” plans using only the Medicare
payments of seniors who, for whatever reason choose to use them?
The answer: Insurer negotiated, lower than “advertised,”
fees for service. Same as Medicare. Add (much) lower private insurer payouts
for drugs and it’s a no brainer. Put Medicare for all or a similar single payer
system on equal footing and we all win.
No comments:
Post a Comment